Register via Eventbrite link here: https://www.eventbrite.co.uk/e/nhs-mental-healthcare-the-erosion-of-compassion-and-empathic-care-tickets-1982678253027?aff=oddtdtcreator
Campaigning for universal Access to Counselling and psychoTherapy
Register via Eventbrite link here: https://www.eventbrite.co.uk/e/nhs-mental-healthcare-the-erosion-of-compassion-and-empathic-care-tickets-1982678253027?aff=oddtdtcreator
Letter from Paul Atkinson to Scrutiny Committees, Healthwatch Committees, Health and Well-being Boards and the Clinical Commisioning Group of the NE London Integrated Care Board area
For the attention of members of the North East London Scrutiny and Healthwatch Committees, and Health and Well-Being Boards
Talking Therapies in the NE London ICB area
I am writing as a Tower Hamlets resident and a psy professional with decades of experience, to ask that you turn serious attention to the accessibility of talking therapy in our communities in the NE London ICB region.
There is a growing crisis, with ever-more people suffering from common mental health distress. At the same time, the NHS Long Term Plan includes promises to reorganise community mental health services. For both reasons, I suggest it is now time for a critical review of the primary care psychological therapies currently being provided by the NHS in the NE London boroughs.
In NE London, as elsewhere, NHS Talking Therapies (formerly known as Improving Access to Psychological Therapies, or IAPT[1]) has for many years been providing an inefficient and unsatisfactory service, supported in part by misleading statistical evidence of its efficacy. Historically, IAPT has not been subjected to independent audit, and its claim to provide a successful, innovative, adult mental health service is neither properly accountable and transparent, nor, in fact, evidence-based. I explain below how this plays out in NE London.
Talking therapy can definitely be brought closer and respond more flexibly to different communities in need of psychological and emotional support. But, to achieve this, the monopoly of NHS Talking Therapies (NHS TT) in primary care will have to be undone. I have set out some of the alternatives in this paper.
The NHS Long Term Plan gives Talking Therapies (TT) three targets: on access, waiting times and recovery.[2]
It does none of these.
2. NHS Talking Therapies is not cost-effective
The cost of NHS TT sessions is not in the public domain, as far as I have been able to discover. But we can do a very crude calculation.
In 2021-22, IAPT funding for NE London was £36.2 million. The median duration of a session that year was 52 minutes, and for a finished course of treatment it was 310 minutes or 6 sessions. If we divide the spend by the number of people who finished a course of treatment (25,275), the cost per session was just under £240.[8]
If we use this admittedly crude measure, NHS TT’s claim to cost efficiency doesn’t hold water. In the Counselling Directory[9] (the largest directory of independent practitioners in UK), over 60 qualified, self-employed, insured and professionally accountable independent practitioners based in east London are currently offering counselling and psychotherapy for under £40 per session.[10] Even allowing for NHS TT’s high drop-out rate of 50% of clients who started therapy, £240 could potentially buy for each patient at least three times the number of sessions.
3. NHS Talking Therapies has an exceptionally high drop-out rate
Why did only 25,275 out of 72,000 referrals in 2021-22 finish a course of IAPT therapy in NE London? What happened to the other 65% of our residents who, for one reason or another, had expressed concern about their mental health?
According to their annual performance data, IAPT services in NE London are more or less average for England as a whole.[11] But, by any comparisons, the dropout rates are exceptionally high.[12]
So, what is the problem with NHS TT?
4. One size doesn’t fit all – the denial of care
NHS TT is a political and ideological project. It is organised around variations of a single psychological theory and practice – cognitive behavioural therapy (CBT). For NHS TT, CBT has been adapted to the requirements of New Public Management in terms of measurable costs and targets, standardisation of practice and data collection, efficient through-put and the prioritisation of utilitarian values.
It has virtually exclusive approval by NICE as evidence-based psychological therapy provision – a status which has been challenged consistently as manufactured and politically protected.[13] Shortly after its introduction in 2008, it supplanted most other counselling and psychotherapy provision in primary care.
Many therapists who are not part of the NHS TT workforce do not recognise its practice as “real” psychotherapy and counselling, in that it does not base itself in the co-creation of a therapeutic relationship and alliance. In many ways, NHS TT offers a technique rather than a relationship; a didactic rather than a therapeutic process.[14] Patients are “told” how to think.
NHS CBT is a model of therapy[15] that certainly helps a proportion of clients with distressing spirals of negative thinking and behaviour. It can be transforming to feel heard, to have the experience recognised and put into words, to have our emotional world taken seriously. For many people it will be their first experience of any kind therapeutic attention. This, in itself, is an admirable achievement of scale by the NHS TT project.
But, for many people and for all kinds of reasons, the NHS TT approach to emotional distress will either not make a connection, or will fail to travel deeply enough to carry meaning for the client. Dropping out is a fact of life for all therapy work, of course, but NHS TT’s lack of relational flexibility, the rigidity of its commitment to an instrumental “assembly line” methodology[16] and its strict adherence to very short-term work[17] puts significant limits on the number of clients who will engage and find it helpful.[18] Moreover, the NHS TT workforce nationally is itself suffering mental health problems under the pressure of delivering “assembly line” therapy.[19]
The service’s monopoly over psychological therapies in the NHS is not based on patient care. In fact, in this period of increasing privatisation and monetisation of health care, it appears to be a forerunner of the politics of denial of care via the rhetoric of data, efficiency and social management.
5. NHS Talking Therapies fail to address inequalities of mental health care
The dominance of NHS TT is an obstacle to responding more effectively to common mental ill-health in our diverse communities.[20] The limitations of the service’s standardised approach are demonstrated, for example, in its limited engagement with mental health inequalities around social deprivation, race and gender.
For example, 72% of less socially deprived referrals who entered therapy in NE London in 2021-22 finished a course of treatment, and 38% recovered. Among more deprived referrals, only 57% completed course of therapy and only 26% recovered. Barking and Dagenham, Hackney, Tower Hamlets and Newham are among the most deprived boroughs in London.[21] In Tower Hamlets, in 2019-20, only 18% of the more socially deprived who entered therapy recovered.[22]
Far more women than men access the service. In 2021-22, 70% of all referrals in NE London and 80% of people who finished a course of therapy were women.
Inequalities of access by ethnicity are striking. My home patch in Tower Hamlets has the largest Bangladeshi population in the UK. Comparing referrals from the Bangladeshi and the white communities in NE London, 36% of all Bangladeshi referrals dropped out before starting any therapy, 47% who did start went on to finish a course of treatment, and only 20% who entered therapy achieved recovery. The same figures for the white population were 28% initial dropout, 54% finished, and 29% recovered.

6. Talking therapy and rethinking community mental health
The NHS’s Community Mental Health Framework for Adults and Older Adults (2019-21)[23] is an ambitious report, promising integrated care in local communities for people suffering severe and common mental health difficulties. But anyone who has been involved with NHS mental health services or who has been campaigning over the years to resist the process of privatisation, outsourcing, defunding, digitalisation and staff reduction will know that we are in a political environment that will not support most of the Framework’s ambitions with the funding and staffing it requires.[24]
Whatever does end up being introduced will almost certainly see the existing NHS TT service being tasked with delivering most of the promised “innovative”, “integrated”, “effective” care. But what does this mean in practice? In fact, NHS TT is highly privatised and heavily dependent on computerised self-help guides and wellbeing apps. It rations access to its services by using diagnostic algorithms and “clusters of unsuitability”. It gives its therapists AI-determined optimal scripts for use with patients.[25] It is one of the few health services that has expanded steadily year on year since its beginnings in 2008.
None of this offers the best way to reach people in distress in our communities. Before yet more money is spent on our local NHS TT service, it needs to be subjected to thorough independent audit. At the moment, it represents an unacceptable waste of resources, while being presented as the only efficient contender in the provision of therapy for common mental health disorders.
Very many psy professionals believe that NHS TT’s approach is neither efficient nor the only contender. There are genuine, viable alternatives that are more likely to help build networks of supportive relationship in local communities.
7. We need diversity of talking therapies
There are many free and low-cost therapy providers in London, run by fully qualified counsellors and psychotherapists, that serve their local community. They are often charities whose funding is limited and precarious.[26] There are also qualified therapists providing therapy and therapeutically-informed support in many community projects.
For example, I have been working for 4 years offering free psychotherapy at my local community centre in Poplar. I am doing individual weekly sessions with an open-ended relational approach. Many of my clients have chronic mental health difficulties but no therapeutic support from local services. I am developing emotional support groups for local residents and a reflective practice group for community workers who are feeling overwhelmed by referrals from GP social prescribing – a Common Mental Health Framework strategy. I have been approached by a local primary school to start a support group for its parents.
I am a founding member of the Free Psychotherapy Network.[27] Many FPN therapists have similar local arrangements with community projects. Our members are involved in a therapy centre at an urban farm in Hackney, free counselling in community centres in Ilford, therapy and emotional support with the homeless and substance misusers in Waltham Forest, work with primary schools and a parent/infant support service in Leytonstone, and a dozen charities offering low-cost counselling in NE London. The picture is similar in other parts of London and the UK generally. At the moment, these projects are small and have minimal funding. With the right support they and projects like them could grow rapidly.
Scores of experienced counsellor and psychotherapist colleagues are interested in working for the common good in community settings, but, unlike me, they cannot all afford to work without funding. Rather than focussing exclusively on funding the expansion of NHS TT with all its limitations, why can we not develop more imaginative and flexible initiatives at a far lower sessional rate? These initiatives could include providing individual and group therapy in community centres, schools and colleges, as well as acting as support workers for residents and the communities around them. The practitioners involved would organise their own supervisory practice and shared peer reflection, make relationships with adult and young people’s mental health care services, community project teams, local schools, GP practices and social prescribers, substance misuse services, homeless groups, and so on.
This kind of model puts therapists much closer to the everyday lives and needs of people, are more open to negotiating those needs with communities and can be an integral part of a bespoke range of ongoing resources and support.
New funding would be great. But there is also money in the system that can be repurposed. We already know of a low-cost counselling service in the Newcastle area that is being partially funded by Primary Care Network social prescribing budgets to provide more relational counselling for clients defined as “unsuitable” by the local NHS TT services. There is even more potential for lasting change if a proportion of local NHS funding that is currently going to our homogenised TT services could be redirected towards the community to deliver on the promises in the Long Term Plan. These NHS budgets could be held by Primary Care Networks, or by individual GP surgeries (who often employed counsellors before the introduction of IAPT) – bringing funding as close as possible to the communities that need to be served.
If the Common Mental Health Framework is to mean anything other than a smoke-screen of words and tech, the role of employed professionals, and their energy for making relationships of different kinds, has to be massively scaled up. Apps and social prescribing to already overloaded and under-funded charities and local authority services is not going to lift our communities out of the mental health crisis we are in. People and relationships built on trust over time are central to any substantive change in the emotional wellbeing of our NE London communities.
8. Audit and scrutiny
NHS TT is regularly praised by its leadership as a major national and international success story.[28]
However, it is not independently audited and relies on the avalanche of its own data collecting to justify and maintain its claims to be a successful, evidence-based service. Many critical reviews of its data suggest a different picture.[29] In terms of its access rate, its drop-out rate and its recovery rate, its performance is poor, and far from cost-effective.[30] As far as the quality of the therapy it provides is concerned, there is no evidence that any positive therapeutic benefit is effective over time. Nor is there any evidence that the prevalence of common mental health problems in the UK population has declined in the decade since the service was rolled out – on the contrary.[31]
I am asking you as members of Scrutiny, Health and Wellbeing, and Healthwatch Committees to give serious consideration to the reality of failings and inefficiencies hiding in plain sight in the spreadsheets of NHS TT reports. In the middle of what seems to be an ever-deepening crisis of mental health, with so much political pressure for cuts in NHS services and staff, and in particular the decades of underfunding and denial of care in mental health care, it is time to attend with the utmost urgency to the need for dramatic improvements in the services available to our residents in North East London.
I look forward to a response from your committee.
Paul Atkinson
Professional Member of the Philadelphia Association
Member of Socialist Health Association/Keep Our NHS Public London Mental Health Group
Member of the Free Psychotherapy Network
[1] Where I refer to the data reports for NHS Talking Therapies before the name change in Feb 2023, I will use the term IAPT.
[2] https://mentalhealthwatch.rcpsych.ac.uk/local-area-reports/detail/north-east-london
https://www.england.nhs.uk/wp-content/uploads/2018/06/the-iapt-manual-v5.pdf pp 36-40
[3] Population of NE London ICS – 2,000,000; adult population = 1,600,00; adult prevalence of common mental health disorders @20% = 320,000 (see https://fingertips.phe.org.uk/profile/common-mental-disorders/area-search-results/E39000018?place_name=London&search_type=list-child-areas); NHS TT target is to give access to 25% of the adult prevalence of common mental health disorders = 80,000.
[4] https://www.bacp.co.uk/news/news-from-bacp/2019/5-december-long-waiting-times-for-iapt-unacceptable/
[5] The definition of “recovery” and the way it is quantified by getting the client to complete a Beck inventory in every session, is a good example of the way the IAPT model has been mechanised.
[6] Some providers’ follow-up to Freedom of Information requests is also non-existent https://www.whatdotheyknow.com/request/following_up_referral_drop_outs#incoming-2084534
[7] https://hrnews.co.uk/nhs-therapists-are-pressured-to-exaggerate-success/
[8] £36.2m/25,275/6 = £238.7 For median duration stats see https://app.powerbi.com/view?r=eyJrIjoiMDk2OWUzMjEtN2YxYS00YzgwLThkMGMtMjNlZWE1MWIyMTk3IiwidCI6IjUwZjYwNzFmLWJiZmUtNDAxYS04ODAzLTY3Mzc0OGU2MjllMiIsImMiOjh9p.32
[9] https://www.counselling-directory.org.uk/search.php?search=East%20London&distance=5&session_type%5B%5D=in-person&session_type%5B%5D=online&business_type%5Bindividual%5D=on&price_min=40&price_max=40
[10] Psychological Wellbeing Practitioners (PWP) who do most of the Low Intensity work in NHS TT have a salary of between £14 and £17 per hour – https://www.prospects.ac.uk/job-profiles/psychological-wellbeing-practitioner
[11] See the March 2023 House of Commons Report for a good national overview of IAPT services – https://researchbriefings.files.parliament.uk/documents/SN06988/SN06988.pdf
[12] In my 40-year experience practising counselling and psychotherapy in independent settings, the drop out rate for more relational therapies, rather than the instrumentalism of IAPT, is likely to be closer to 10%. However, studies of dropout rates in different settings and environments of mental health services are complex and vary. By any comparisons, IAPT dropout rates are exceptionally high – see https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-019-2235-z,https://cpe.psychopen.eu/index.php/cpe/article/view/6695/6695.html,https://onlinelibrary.wiley.com/doi/abs/10.1002/capr.12249, https://iaptus.co.uk/2022/06/what-impacts-patient-engagement-with-mental-health-treatment/
[13] http://www.limbus.org.uk/cbt/index.html
[14] https://www.bmj.com/content/380/bmj.p464
[15] https://www.england.nhs.uk/wp-content/uploads/2018/06/the-nhs-talking-therapies-manual-v6.pdf p.13. In NE London ICB in 2021-22, there were 9920 finished courses of CBT; 6365 of guided self-help (book); 1835 counselling for depression; 1365 non-guided self-help (book); and a small number of other types of therapy – see https://app.powerbi.com/view?r=eyJrIjoiOTIyYTgyYjEtM2QxZS00YzYyLWI3YTEtZDU1NjhjNjlmYmE0IiwidCI6IjUwZjYwNzFmLWJiZmUtNDAxYS04ODAzLTY3Mzc0OGU2MjllMiIsImMiOjh9p.4.
[16] https://www.pccs-books.co.uk/articles/article/the-industrialisation-of-care-counselling-psychotherapy-and-the-impact-of-i
[17] This therapist can simply not understand how, in many cases, “courses of treatment” consist of just two sessions.
[18] https://bpspsychub.onlinelibrary.wiley.com/doi/10.1111/bjc.12314
[19] https://www.rcpsych.ac.uk/docs/default-source/events/faculties-and-sigs/general-adult-psychiatry-20/research-case-reports/abeku-koomson.pdf?sfvrsn=76850f44_2#:~:text=Amongst%20the%20IAPT%20workforce%2C%20PWPs,in%20the%20mental%20health%20field2 http://www.cbtwatch.com/nhs-talking-therapies-on-the-brink/
[20] Its influence is not confined to NHS services. Its model of therapy practice has been imposed on most charitable therapy provision that relies on public and charitable funding. MIND and other major mental health charities have, in fact, become NHS-approved IAPT providers.
[21] https://centreforlondon.org/blog/deprivation-london/
[22] https://www.health.org.uk/news-and-comment/charts-and-infographics/referrals-for-psychological-therapy-from-patients-in-deprive See NE London ICB survey of the scale of deprivation and mental ill-health here – https://www.northeastlondonhcp.nhs.uk/downloads/Insight/NEL-Population-health-profile-May-2022-v4.pdf
[23] https://www.rcpsych.ac.uk/docs/default-source/improving-care/nccmh/the-community-mental-health-framework-for-adults-and-older-adults-full-guidance/part-1-the-community-mental-health-framework-for-adults-and-older-adults—support-care-and-treatment—nccmh—march-2021.pdf
[24] For example, Prof Peter Fonagy, UCL and NE London ICB partner, recently wrote: “A continuing challenge lies within resources – it is estimated that if every psychologist worked 50 hours a week they would still only meet 12% of the current demand.” https://uclpartners.com/blog-post/meeting-mental-health-needs-with-innovation-and-connection/
[25] https://www.lyssn.io/press-release_trent-pts/
[26] https://freepsychotherapynetwork.com/organisations-offering-low-cost-psychotherapy/
[27] https://freepsychotherapynetwork.com/
[28] https://www.england.nhs.uk/blog/iapt-at-10-achievements-and-challenges/
[29] http://www.cbtwatch.com/clinical-commissioning-groups-ccgs-incredibly-naive-re-iapt/
[30] See NE London ICB report p.12 – https://northeastlondon.icb.nhs.uk/wp-content/uploads/2022/07/Annual_Report_2021-22_FINAL_Redacted.pdf
[31] http://www.cbtwatch.com/more-treatment-but-no-less-disorder-what-is-going-on-here/ Compare 2007,2014,2017 – https://app.powerbi.com/view?r=eyJrIjoiMmRiY2FkYmUtZDQwOS00MDNlLWEyYTktZTQ1N2RiZTNkNGM5IiwidCI6IjUwZjYwNzFmLWJiZmUtNDAxYS04ODAzLTY3Mzc0OGU2MjllMiIsImMiOjh9and https://fingertips.phe.org.uk/profile-group/mental-health/profile/common-mental-disorders/data
Therapists Against the Work Cure
Statement from Partners for Counselling & Psychotherapy (PCP) 13th October 2022
On Monday 10th October 2022, World Mental Health Day, the Government announced £122 million of funding for mental health. But the bitter reality is that this money is not being spent on in-patient beds, community mental health initiatives or trained counsellors and psychotherapists for public mental health services. Instead the Government is using this money to recruit and train 700 ‘employment advisers’ to work alongside therapists in the NHS’s flagship Improving Access to Psychological Therapies (IAPT) programme. This will help drive the highly contested policy of ‘welfare conditionality’ that threatens benefits claimants with sanctions if they don’t conform to certain patterns of behaviour, a policy which targets the poorest and most deserving sections of our society at a time when they need the greatest help.
Despite the timing of the press release, the money announced is not being used to build mental health support. Instead it is an expansion of an existing IAPT-based scheme providing, as the announcement states, ‘combined psychological treatment and employment support to help [people] to remain in, return to or find work and improve their mental health’ {1]. The linking of work and mental health, however, is deeply problematic. In 2015, hundreds of counsellors, psychotherapists and academics opposed the pilot scheme that first put together Jobcentre employment advisors and IAPT therapists, a scheme that in a letter to the Guardian [2] the signatories denounced as anti-therapeutic and professionally unethical.
Nothing has changed except that this policy now threatens to coerce a greater number of people into a system of employability interventions and psychological treatment in order to avoid sanctions on their welfare payments, including the main disability grants. As the highly contested Universal Credit programme is rolled out across the UK in response to rapidly growing low pay and job insecurity, many more people will be unable to secure living wages and will be forced into the benefits regime, where they will be subject to this pressure to undergo combined psychological interventions and employment advice.
What is the role of therapists in such a system? For us, work is not a health outcome. Employment is not an expected or even inherently desirable result of genuine counselling and psychotherapy. Real therapy does not aim to return individuals to the workplace or to keep them in jobs that may be economically insecure, psychologically toxic, systemically oppressive and personally damaging.
The linking of State therapy and employment advice, particularly if connected in any way with a punitive benefits system that has the power to sanction claimants for their perceived failures to find work, must surely contaminate some of the central tenets of good therapy – not least the autonomy and right to self- determination of the person undertaking it. The rolled-out scheme may be trailed as ‘voluntary’ but if ‘employment advisers and therapists will work together so that a person can return to or find work easier and faster’, as the Government say, then the non-coercive integrity of the therapy cannot realistically be maintained.
Given that the Government statement is at pains to point out how the overall aim of the project is ‘driving economic growth’, we also have to ask therapists whether they can – ethically and in good faith – align their practices with such an agenda. The therapist’s job is not to work from an assumption that ‘work is good’ or to aim to reduce the number of people receiving benefits, including disability benefits that are increasingly claimed on the basis of mental illness, but to provide an opportunity for reflection on all aspects of a person’s life.
As a network of organisations representing counsellors and psychotherapists, we at PCP believe that this announcement on World Mental Health Day is a cynical attempt to reduce government spending at the expense of people who most need genuine therapeutic support during an unprecedented period of economic crisis. We reject the financial logic that underpins the linking of employment and wellbeing services as it is a profound attack on the principles of talking therapies and will lead to a cruel and measurable deepening of the UK’s mental health crisis.
Partners for Counselling & Psychotherapy
http://www.partnersforcounsellingandpsychotherapy.co.uk
email: admin@partnersforcounsellingandpsychotherapy.co.uk
twitter: @pcp_uk #workcure #psychocompulsion
Register via Eventbrite link here
After the big response to our launch event in January, it’s been hard working out how to encourage people to get together and organise campaigning action in support of the uACT manifesto. Actively campaigning for change is always a struggle, there are several existing progressive groups campaigning around many of the issues and the general political environment is pretty antithetical to the possibility of political hope and social change.
It is clear, however, that there is an appetite among therapists and other psy workers to stand up for the value of relational work with therapy clients as well as in wider community settiings, and to oppose the dominance of transactional and medicalised “management” of our society.
This meeting is for people who want to build and support campaigns aimed at challenging forms of psy practice that essentially manage and maintain social and emotional injustices as part of a system which routinely and irresponsibly puts money before people, and does not pay attention to the very real social struggles that affect our clients and their mental health.
So far, suggestions for campaigning have included:
– concerted exposure of the failures of the IAPT service by local groups through:
– developing alternative proposals for relational therapy provision in the community, among young people, at schools and colleges and so on
– supporting campaigns to stop SCoPEd; to undo the hegemony of medicalisation, diagnosis, bio-chemical ideologies and short-term behavioural therapy; to challenge phoney definitions of evidence-based modalities of therapy; to put a halt to unpaid jobs in counselling and psychotherapy; to challenge IAPT barriers to NHS work; campaigning for social justice and diversity in our training curricula.
– public events like a People Not Pathology national conference; press releases; a progressive Youtube news channel on “mental health” issues with interviews across a range of activity and experience in the field.
We are hoping represenatives from some of these campaigns will come to the meeting and speak briefly about their work. But the focus will be on people attending who want to get involved in campaigns, who have ideas for organising action and for promoting the availability of counselling and psychotherapy and other forms of relational psychological support across society.
We will organise the meeting to offer participants the maximum opportunity to get together to speak, discuss and make decisions for the future.
We hope to see you on the 15th.
All the best from the uACT organising group
ua2counandt@lauras1990
Hello uACT,
I am certainly one of those wondering what I can usefully contribute to uACT. But first thank you all for the work you and your colleagues put into the launch. I particularly valued James’s slot, which provided a very clear analysis of what’s going on and how much worse things have become in the last decade and a half. I have since got hold of a copy of ‘Sedated’ which gives a brilliant account of the mess in which we find ourselves. I like it – it’s more sophisticated than the stuff we used to produce in the Alliance.
And my apologies for taking so long to get back to you. What follows is my perhaps rather gloomy assessment of where the best opportunities for uACT lie now. No doubt most of it will be familiar to you. The short version is that I’m inclined to believe, as was said during the launch, that uACT needs to be ready for a long haul.
As for the counselling and psychotherapy world, one of the changes that struck me over last 15 years since Alliance was formed is that of growing fragmentation. Advertised trainings it seems increasingly focus on additional qualifications rather than on reflection, interesting questions or a deeper understanding of what therapy is. This fragmentation is of course also driven by practitioners’ keen desire to generate a viable income.
This fragmentation of counselling and therapy into separate specialist subject areas is also driven by funders who focus in ever more detail on outcomes – in other words they focus on the fixing people and their problems aspect of therapy. As a result we get Student Wellbeing Services rather than student counselling; a move away from the talking therapies in drug and addiction agencies in favour of more tightly targeted initiatives; the plethora of interventions IAPT covers in order to address anxiety and depression; and so on. What I’ve noticed as a supervisor is that these specialisms tend to draw practitioners deeper into the fixing people and their problems dimension of therapy at the expense of considering life satisfaction and meaning making. As a result all too often practitioners feel over responsible for fixing things. In this they are aided and abetted by their clients’ expectations as well as by their managers, who themselves can overload them with too much work so that creativity and reflective thought gets pushed to one side in favour of meeting targets. Nowadays the difficulties that supervisees bring to me very often revolve around them not having enough mental space to be able to step back and think.
Such fragmentation is further facilitated by managers who want power, status and money for themselves, their organisations and their members. BACP seems to be redoubling its efforts in this respect. It buys into the rhetoric, irrespective of whether the rhetoric is intellectually credible. Sometimes I wonder how much of this obfuscation is deliberate and dishonest. Mostly I think they just can’t afford to pay attention to gaps and inconsistencies. Hence SCoPEd, its engagement with argument about evidence based treatments, DSM – and so on. The BACP supervisor competencies focus only on the supervisory dyad and omit anything else – no mention of peer supervision, group supervision or any grasp of the wider context within which the work takes place. From one point of view I find this narrow perspective astounding, but given BACP’s priorities I suppose it’s entirely predictable.
My experience of teaching on a counselling diploma course is that most of the students are overwhelmingly focused on establishing their careers and on earning an adequate income. They are reluctant to adopt anything but a deferential attitude to professional bodies and their requirements. This includes avoiding adopting critical views of these bodies – they find this simply too stressful. They want to pay their annual membership fees, tick all the relevant boxes and not think any further.
As a result at some level or another they buy into all the received wisdom about qualifications, hours of training, hours of practice, hours of supervision, the need for further certification and so on – none of which is ‘evidence-based’. On the other hand they also buy into NICE guidelines, IAPT and ‘evidence-based’ approved therapies.
In order to establish themselves they have to jump through innumerable hoops. In the first place they have to establish that they have enough preliminary experience to be accepted on to a training. After that they have to find a suitable placement where than acquire enough practice hours in order to qualify. Once qualified they have to acquire further (usually unpaid) practice hours in order to gain accreditation. At some point many will start a modest private practice, which will generally take a few more years to establish.
At a later point, perhaps a decade or so after embarking on this journey, some practitioners find they have a thriving practice. It’s at this point I have found I have more productive conversations with supervisees. We can more easily talk about aspirations and ideals, about being confident about being able to earn an adequate living whilst also achieving a satisfactory life/work balance, about continuing to learn and develop, about keeping their curiosity and enthusiasm alive, about making a contribution to the future of the planet and the wider society – and about whether they need to stay in hock to a professional association like BACP. Answers to this last question vary to some degree depending on how old the supervisee is. Those who are within a few years of retirement tend to have more confidence about breaking free of bodies like BACP. Others have longer to wait and find it more difficult to predict the future legislative environment.
uACT challenges all this received wisdom. It asserts the crucial importance of being able to bring questions of life satisfaction and meaning making into therapy, because otherwise it’s all too easy to find that nothing makes sense. But I can’t see government ever whole heartedly buying into funding ‘real therapy’ – they just want narrow problem areas fixed. And yet it’s vital that the vision that uACT stands for is kept alive for future generations. uACT is one of the strands in this longer term view as are, amongst other bodies, IPN and the PCU.
Perhaps our field of work is dividing into two. One of these is funded by the state in order to ‘fix’ people in an increasingly professionalised manner, while the other – represented by those drawn to uACT – is more collaborative and addresses the questions that arise when the work moves beyond fixing people, whether or not the fixing has been done. Fixing people now requires endless further specialisation (eg therapy for young people, for people with eating difficulties, for people addicted to one thing or another, for people who are traumatised as well as people with anxiety or depression)
In some ways I am reminded of where the therapy world was in the 1980s when they was an energy and enthusiasm for exploration and curiosity, but where there was little in the way of funding or employment for practitioners. Initiatives came from grassroots organisation and voluntary endeavour. It may be that ‘real therapy’ will be strongest in private practice and counsellors and therapists will need to be encouraged to think about what they can provide, as in FPN and similar initiatives. My own energies recently have been tied up with the attempted revival of IPN as a base in which critical thinking about therapy can find expression.
To preserve my sanity most of my time and energy is increasingly focused on things closer to home – my friends, my family and especially my granddaughters as well what I want to do before I become too decrepit to enjoy very much. Even so I will keep talking to colleagues about uACT and its vision.
All best wishes to you, Paul, and everyone active within uACT,
Arthur Musgrave April 2022
‘I think the kids would be dead now if I hadn’t come to NEWPIN.’ Mother
What help is there for parents at their wits’ end? Who is there to give long-term support? Who can transform their lives and save their young children from physical and emotional harm? Who can provide the right sort of service to ensure that the parents don’t end up dead, or in prison or psychiatric hospital, and the children in care?
An answer
NEWPIN, New Parent Infant Network, can. The first NEWPIN centre opened in south London in 1982. Anne Jenkins, a health visitor, knew that what she could offer to distraught families was nowhere near enough. The service she developed is described by a NEWPIN co-ordinator in Australia as ‘the most unique, special, effective, empowering, life-changing, authentic change programme for families in the world.’ John Bowlby was ‘a great fan.’ And a mother who went through it calls it ‘a miracle.’
Imagine….
Just suppose you are a mother or father with at least one child under five, who is finding life impossibly difficult. You feel depressed or anxious most of the time. Your relationships with your children, partner, if you have one, maybe your own parents, are fractured and always have been. You probably didn’t have the best childhood yourself. You can’t bond securely with your kids. You hate yourself and sometimes everyone else too. You’re in daily despair with no idea what to do or where to turn.
Hope
Then you hear about NEWPIN. You meet the co-ordinator to discuss if you want to change and are willing to involve yourself about twice a week for a year or two in a challenging programme. You decide to give it a go. One of the regular members becomes your befriender, visits you and accompanies you to the centre, and helps you settle in. You find the other parents and the staff welcoming, kind and in no way seeming to judge you. Your child gets used to the playroom, makes friends and finds respite from tensions at home, while you relax and have a cuppa in the living room with the other members who seem to take a genuine, understanding interest in you. This is a new experience.
The challenging programme
Once you’ve settled, in a few weeks’ or months’ time, you join two regular activities: the therapeutic support group, run by a group analyst, and the personal development programme, where you learn more about every aspect of life as a parent. The co-ordinator is probably a woman who needed NEWPIN herself and now has a paid position: you never sense she’s looking down at you. For the first time you find yourself expressing your feelings and revealing your vulnerabilities, your history, your day-to-day struggles without anyone being shocked or critical. In fact, all the others have their own, often similar, stories. You no longer feel isolated or hopeless. Your self-esteem and confidence grow. You gain insight into why you find life so difficult as you recount your earlier experiences; and in the playroom you learn, with the play facilitator, how to play with your child and develop a healthy attachment. If you feel the need for one-to-one counselling, it’s provided. There’s a 24-hour helpline.
Your future
Once you’re happier, more stable, able to relate well to others, you can be allocated a new member and become a befriender yourself. Perhaps in time you could train to be a NEWPIN co-ordinator. You see a positive future, maybe through further education or vocational training. NEWPIN guides you while you find what’s right for you. You emerge as someone who appreciates and understands herself and her children, and the enormous gift that NEWPIN has given.
NEWPIN in the UK and Australia
Flourishing NEWPINs operate in Derry (Northern Ireland) and Westminster (London.) There are also some part-time centres in Wandsworth (London.) There is a growing number in Australia.
The urgent need for more NEWPINs
The Covid pandemic has seen a dramatic increase in domestic violence, isolation, and the neglect and abuse of children. This makes it all the more vital to provide a NEWPIN centre everywhere for those parents who are able and willing to engage with it. Moreover, NEWPIN saves huge amounts of future public money and personal tragedy. As a parent and a psychotherapist, I know how hard it can be to be a ‘good enough’ parent and was privileged to help set up a Newham NEWPIN in 1992. I now want to press for the establishment of many others.
‘What sticks out about NEWPIN from all the other places we send people to is that it works.’ Social worker
To learn more
If you would like to know more, or might even be interested in helping to set up a centre, do get in touch. The booklet The Miracle of NEWPIN is available from the address below for £5 including postage (please make cheque payable to Ros Kane): Ros Kane, 15 Matcham Road, London E11 3LE roskane@btinternet.com 0208 555 5248.
About the author
I grew up in north London suburbia with parents with a Communist Party past. Meeting anarchists later on gave politics a new twist which has persisted, depite joining the Labour Party when Corbyn became leader. After a long stint of paid employment such as social work, prison work, and campaigning to abolish prisons (!), I trained at the Guild, and set up charities to help children’s emotional health. I now devote most of my work time to completing two volumes of ‘Nothing More Important’ about preparing kids at school to be good parents, trying to set up more NEWPIN centres, and seeing a few free or low-cost patients. The charity Carefree Kids showed that volunteers – many without formal qualifications – could do effective, affordable work in schools as therapeutic play workers.
This is a reworked version of a talk I’ve given on a couple of occasions, most recently at the National Counsellors Day conference in June. I am writing as a member of the Free Psychotherapy Network (FPN) and the campaign for universal Access to Counselling and psychoTherapy (uACT), but the responsibility for the opinions expressed is mine alone.
Is there a mental health crisis?
I think we probably have to allow that there is a mental health crisis of some kind going on in the UK, and by the way, all around the globe, it seems.
In the form I am meaning mental health crisis here, it is a relatively recent phenomenon. I am thinking, for example, of how often we hear about people’s mental health in the Mainstream Media (MSM), and also perhaps especially on social media, particularly if you are plugged into the mental health/therapy/service user echo chamber – as many of us are these days.
I recently had a go at gauging how often “mental health” and “mental health crisis” were mentioned in the press, in MSM headlines, and how the number of mentions has mushroomed over recent years. It was a very sparse, quick survey in the end, but nevertheless quite dramatic.


Since the financial crash in 2008, there have been regular headlines about the state of mental health among young people, especially women, about eating disorders, suicide, self-harm as well as depression, anxiety and anti-depressant prescriptions:



And there has been a proliferation of celebrity mental health reports, with confessional headlines from across the spectrum:


What is this mental health crisis about?
But what is this mental health crisis about? What is it saying about our society and our changing relationship with emotional life, the priority we are giving to our own and other people’s psychological experience and pain?
It’s clear that awareness of mental health issues has been rapidly growing across the globe. As well as media coverage, there have been scores of reports in this country from charities like MIND and many others, the Royal College of Psychiatrists, central and local government and so on. Similarly from Europe (eg OECD reports) and more widely from the World Health Organisation – all pronouncing on the increasing incidence of common mental health conditions like depression and anxiety. It’s now everyday among younger people in the UK to be talking about their experience of MH problems and their diagnoses.
The Improving Access to Psychological Therapies service, introduced in 2008, has changed the scene as far as common mental health (CMH) conditions and their treatment is concerned. Since 2014, over 1 million people a year have been referred, or have self-referred, to IAPT. In 2019-20 there were 1,700,000 referrals.
We might expect then that all this media coverage indicates a reduction in social stigma around mental health problems. After all, almost every news report these days seems to include mention of the mental health dimension of the item covered. On Radio 4 as I write this paragraph, the BBC is reporting “a survey of 4000 people on the cost of living. 56% reported cutting food and car journeys. Two-thirds said their MH had been affected.”
But things are not so simple. There is a significant stigma still in relation to psychosis, especially diagnoses of schizophrenia. There’s certainly stigmatisation of people in marginalised communities like the homeless, substance misusers, people experiencing poverty or disability – and severe and enduring MH conditions generally. And of course, if you are black or brown there is always likely to be a stigma.
There are also differences in levels of stigma within minority ethnic communities.
And we might ask, does the language of mental health and medical model diagnosis translate into awareness of psychological life, feelings, relational dynamics and the dynamics of power?
Is there MORE psychological distress and suffering in recent decades than in the past?
This is a difficult one. Firstly, we have very little comparative data before WWII. Data begins to really take off from the 1970s when anti-depressants begin to hit the consumer market and behavioural scientists and clinicians begin the big randomised controlled trials of behavioural therapy – notably Aaron Beck, “father” of cognitive behavioural therapy (CBT).
The beginnings of so-called “evidence-based psychological treatments”, the mental health market and the mental health crisis are chronologically coincident. From a different angle, we might add to this, as far as increasing awareness is concerned, the role of humanistic growth movement therapies and alternative cultures around mind, body, spirit therapies from the late 60s and 70s.
Psychological trauma and distress, depression and anxiety, are not something new. We human beings have forever been living in societies that normalises oppression and exploitation, through a combination of brute violence on the one hand and cultural narratives of “there is no alternative” on the other. Going back over the last century or two, I don’t imagine that the emotional and psychological stresses of ordinary people’s lives have been any less violent and traumatising.

For the political class, it has always been important to minimise and/or deny the damage we are doing to ourselves and our world in the name of necessity, in the name of maintaining the known and familiar (the status quo), or carrying on in the name of progress or economic growth.
There is however evidence that in certain respects psychological suffering is on the increase.
As far as the prevalence of CMH problems is concerned, government statistics report that there has been an overall increase in the prevalence of common MH problems between 1993 and 2014.

It’s not clear though how far this chart illustrates growth in actual distress and growth in consciousness around valuing of the awareness of distress.
There certainly seems to be an increase in MH problems among young people, girls and young women in particular.

The number of A&E attendances by young people aged 18 or under with a recorded diagnosis of a psychiatric condition more than tripled between 2010 and 2018-19.
7% of children have attempted suicide by the age of 17. 72% of those in suicide counselling with NSPCC are girls.
26% of young women experience a common mental health problem, such as anxiety or depression – almost three times more than young men.
Suicide is the single biggest killer of men under the age of 45. And a marked gender split remains. For UK women, the rate is a third of men’s: 4.9 suicides per 100,000.
There is also some evidence that the number of people suffering Severe Mental Illness (SMI) is on the increase.
There is another way of looking for the meaning of the MH crisis: the social determinants of people’s distress and suffering
Let’s start with an understanding that life itself is difficult and stressful, that we are all physically, emotionally and spiritually vulnerable creatures whatever else, some more so than others at different times and in different places, and we need each other’s empathy, understanding and practical support to get by.
But this is not the way our society is organised. On the contrary, we are living in a society that generates misery, anxiety, loneliness and depression.
As a socialist, I’d argue that the MH crisis is a crisis of capitalism, in other words, it is a systemic crisis around the power relations of class, race and gender, a crisis of alienation through the transactional worlds of markets and money, a crisis of exploitation and the extraction of resources, a crisis of greed and inequality, a crisis of the undermining of community and of social relationship generally.
Just as modern capitalism is driving us towards a breakdown in our relationship with the natural environment, it is driving us towards a breakdown in our relationship with our emotional and psychological environments, our bodies and each other.
It is generally acknowledged by most academics, policymakers as well as activists that the social conditions of people’s lives have a critical causal impact on the levels of stress, anxiety and depression they experience. More importantly, it is just plain common sense to most of us.
One of the most recent and extensive examinations of the social determinants of mental health in the UK is the Marmot review 2020. Michael Marmot compares the state of UK society ten years after his previous report on the social iniquities of health. He reports on the major inequalities in socio-economic conditions contributing to disparities in physical and psychological health in the UK. The catalogue of social determinants includes inequalities of income and wealth, poverty, household debt, lack of decent housing, welfare cuts, food and fuel insecurity, lack of social mobility and equal opportunity, racial discrimination, sex and gender discrimination, adverse and abusive working conditions, childhood poverty and adverse experience.







A few years ago, Psychologists for Social Change spelt out the emotional impact of austerity polices on ordinary people like this:

And more recently, Jack Munro has described the link between poverty and psychological distress with passion in the Guardian:
“The 14.5 million people living in poverty in the UK today are ticking time bombs of increased toxic stress, post-traumatic stress disorder, CPTSD, cognitive difficulties, depression, gum disease, chronic fatigue, osteoporosis, asthma, chronic obstructive pulmonary disease, arterial disease, mental illness, diabetes, hypertension, inflammation, autoimmune disorders, suicidal ideation and suicide.”
What would follow from all this for any government or policy maker really concerned about the MH of the country is that addressing socio-economic iniquities via social policies like a basic living income and adequate housing for all, equality of opportunity through education, a proper social security safety net, redistribution of wealth and income via progressive taxation etc – these are the essential changes we need to become a more secure, confident, emotionally open and relating society.
In fact, we have seen the opposite – since the crash government policies have prioritised wealth accumulation by a minority at the expense of the social, material and psychological well-being of the majority, culminating in the austerity policies introduced after 2010 which have utterly immiserated the most deprived areas of the country.

The reality of the government’s concern for the UK’s mental health crisis: managing the dysfunctional system of modern capitalism
In fact, while we are ostensibly in the midst of a MH crisis, and governments have been raising the alarm and talking about more resources for MH services, more staff, more community MH, parity of esteem – the same governments have in fact been cutting MH services, cutting beds, imposing real pay cuts, and accumulating staff vacancies.
The total number of mental health nurses in NHS England is down by over 3,000 in real numbers since 2009. Between 2009 and 2020 there has been a 12% drop in the number of mental health nursing posts.
Anyone with severe and enduring MH issues looking for support in the community will know that resources, ongoing professional support, decent housing, a reliable relationship with a key/social worker/psychiatrist are just not available.
Both the climate and MH crises are symptoms of a systemic breakdown in our society. Both have the power to turn our world upside down. Both are being managed as if they are unfortunate but inevitable consequences of progress. Both are being approached by the political class with disingenuity and duplicity. It is increasingly clear that people with power and money do not actually care about the lives of ordinary people. Both require social and political transformation.
As far as common MH conditions are concerned, instead of responding to the growth of symptoms of distress and inability to cope as a signal of something dysfunctional in the way society and the political economy are organised, the problem has been defined and responded to as the dysfunction of the individual.
So, for many of the more establishment commentators on the social determinants of mental health, social factors may determine the conditions which are likely to promote MH problems, but the causes of each person’s symptoms lie in their individual predisposition to mental ill-health – bio-chemistry, negative cognition, negative behaviour.
The current state of denial of systemic crisis is demonstrated in the term – mental health crisis. Mental health is a misnomer. First, the emphasis on cognition implied by the term “mental” is deeply unsatisfactory in that psychological life is much more about the dynamics of an emotional relationship, unconscious life, fantasy, dream, and embodied experience as anything mental or cognitive. Second, applying the medical model of health and ill health to psychological experience implies a norm of healthy psychological life, and the pathologising of so many everyday dimensions of the human condition – depression, anxiety etc. loneliness, sorrow, defensiveness, paranoia, euphoria, the multiplicity of the self – that might conflict with the one-dimensional narrative of normalcy within the frame of neoliberal values.
Put another way, the term mental health is also a POLITICAL misnomer. It is however the most generally acknowledged language of psychological life and suffering.
If unhappiness and emotional pain are illnesses of the individual, they can be treated under the medical model through scientific investigation, evidence-based diagnosis and treatment plans with the goal of getting us back on the horse of normal, healthy life – or offering us an understanding that if we cannot, it is our individual insufficiencies and weaknesses that are at fault.
Lord Richard Layard, co-founder of the IAPT service and Tony Blair’s Happiness Tsar, helped set up Action for Happiness in 2010. The front page of its website used to picture its understanding of the causes of unhappiness like this:

It’s a telling image. 50% of our happiness or unhappiness is rooted in our individual genetic make-up, the social determinants of happiness account for only 10%, and 40% can be influenced by cognitive or behavioural action.
The IAPT service, informed (loosely no doubt) by this kind of “evidence-based finding” is an excellent example of an approach to mental health that confirms that there is a crisis, that the crisis is based on the unhealthy mentality of individuals, and that it can be diagnosed and fixed without changing the fundamental structure of society.
Since its rollout in 2008, the number of people referred to IAPT has grown to 1,700,000 in 2019-20. IAPT currently treats people for depression, anxiety, a dozen categories of physical, emotional and behavioural disability, psychosis, OCD, several phobias, Long Term Conditions like IBS, obesity, chronic fatigue, PTSD, and body dysmorphia. It has an official budget of £700 million this year.
Current estimates of the prevalence of CMH problems in England put the figure at 20-25% of the adult population who will each year experience a diagnosable condition. IAPT is required by the government and the NHSE to offer access to psychological therapies to a quarter of that prevalence in 2021-22, a total of about 1.5 million adults. It is also required to achieve a 50% recovery rate.
What is so telling is that by the standard of its own targets, it is a total failure. If we look at last year, though it had 1,700,000 people as referrals (over the 1.5 million target) only two-thirds started a course of treatment, only a third completed, and only 16% of the original 1.7 million recovered. In areas like Manchester, the picture is significantly worse. Only 7% of its original referrals recovered.


If only a third of people applying for access to IAPT therapy 40% of the 1.5 million target) actually, complete a course of treatment, can we then claim that we have offered access to therapy to 1.5 million people? If only 16% of those applying for therapy end up being successfully treated by IAPT’s measure of success, can we really claim a 50% success rate? I don’t think so.
Despite all its claims to have transformed access to therapy on an unprecedented scale, IAPT is in reality a grossly ineffective and wasteful use of NHS resources. In fact, I think it would be fair to say that its primary role is political rather than therapeutic, namely to manage on behalf of the state a severely dysfunctional and sick social system, and to disguise this unwholesome fact with a smokescreen of diagnosis and cheap behavioural “solutions”.
Campaigning with uACT
No government or political party in modern Britain has so far prioritised the basic material, relational and emotional needs of the people over the interests of capital. Social and economic policies have therefore consistently carried a cost of harm to the psychological welfare of the many in the interests of the few. Unless and until this changes, government mental health policies are likely to be taken up with attempting to mitigate the damage it is itself inflicting on the society it purports to serve.
At the heart of the uACT campaign is the understanding that the fundamental problems facing us as a society, and perhaps particularly as therapists, is the fact that we are becoming an increasingly transactional, managed society. Human relationships are being stripped out of our public lives at a rate of knots. The inequalities and suffering in our society are being treated as problems to be addressed piecemeal by technical and administrative strategies that reduce us as human being to data and data management.
In the world of counselling and psychotherapy, IAPT and the reforms currently being introduced in the NHS are at the cutting edge of building a society in which open-ended mutually respectful relationships between people are being reduced to behavioural and financial transactions.
UACT is a campaign for the promotion of universal access to open, democratic and mutually respectful relationships within counselling and psychotherapy, and in a wider sense, it’s also a campaign for community and relationship at the centre of society and our politics as a whole.
Join us.
Paul Atkinson June 2022
ua2counandt@gmail.com
Date: 09-Mar-22
Time: 19:00-20:00 (plus a bit extra!)
Attendees: Andrew Hoyt, Andy Whitehouse, Becky Goodwin, Chris Grieve, Ellen Boyle, Gram Davies, Marsha Oza
Notes taken by: Marsha
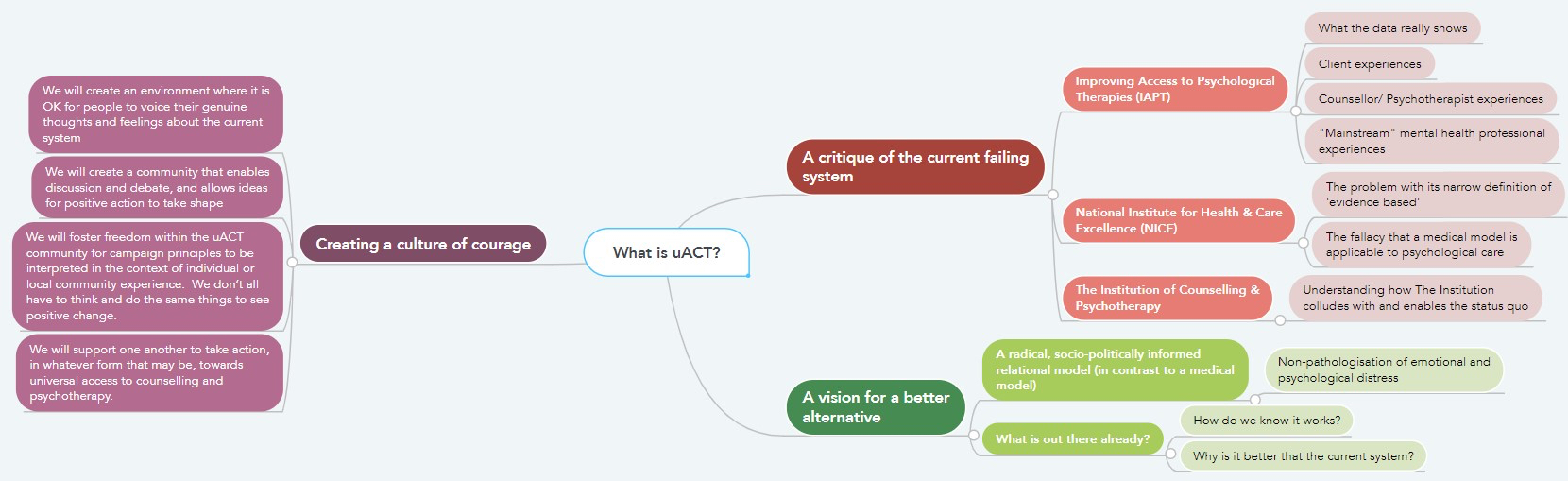
We used the time to meet one another, and share thoughts about the campaign, particularly with regards training/ trainees. Many of these mirrored/ supported ideas from the organising group expressed in the attached graphic (which has been slightly amended since the first iteration following a suggestion from Becky to describe “a radical, socio-politically informed relational model (in contrast to a medical model)”, which I didn’t think anyone would argue with!).
Thoughts from the group about what we’d like to see as follows:
Becky to organise. Date and time tbc.
by Jay Beichman
Evidence-based medicine can be conceptualised as a three-legged stool in which ‘the use of evidence (first leg) is to be balanced with the expertise of the clinician (second leg) and characteristics and context of the patient (third leg)’ (Wampold & Imel, 2015, p. 11). It has been further described as making ‘use of individual patients’… preferences in making clinical decisions about their care’ (Sackett et al., 1996, p. 71). Sackett et al. (1996) warn that ‘without clinical expertise, practice risks becoming tyrannised by evidence, for even excellent external evidence may be inapplicable to or inappropriate for an individual patient’ (p. 72). It is important to note that in these conceptualisations of evidence-based medicine, which are mostly sympathetic to and uncritical of it, evidence is not seen as superior to ‘clinical expertise’, and it is also not seen as superior to patient choice. Yet arguably, in the practical application of evidence-based medicine, it seems as if two legs of the stool have been taken away, with just the first leg (that of evidence) being considered, with the wishes of clinicians and patients being demoted if not forgotten. This was how some practitioners viewed the impact of evidence-based medicine in the USA, and it is also how many practitioners began to view it in the UK, especially since the establishment of the National Institute for Clinical Excellence (NICE) in 1999 (its title was later changed to the National Institute for Health and Care Excellence, but it uses the same abbreviation).
NICE states that their aim was ‘to ensure that the most clinically and cost effective drugs and treatments were made available widely on the NHS in England and Wales’ (NICE, 2016, online) and to ‘speed up the pace at which good value treatments were used’ (ibid.). They also claim that they ‘established a worldwide reputation for producing authoritative, evidence-based advice and guidelines’ (ibid.). In this self-appraisal it is worth noting the casual use of the phrase ‘evidence-based’, which has fully seeped into everyday discourse and is used, without any need of explanation or critique, throughout the media. Everyone knows, or thinks they know, what it means. It is also worth noting the managed-care implications of ‘good value treatments’ putting the cost of treatments as a central concern. NICE is, unsurprisingly, supportive of the medical model, and this necessarily has implications for the provision of therapy. Therapy was perceived by NICE as a medical treatment like any other, and it seemed as if therapeutic practices were shoehorned into the medical model, without any consideration that they might not be as straightforwardly understood in the same way as drug treatments or medical devices.
This is partly due to NICE’s privileging of RCT evidence over any other kind (see, for example, NICE, 2014/2017, p. 103 cited in Barkham et al., 2017). The BACP in its response (BACP, 2017a) to the NICE draft guideline for depression note that RCTs are seen as superior to even the ‘very large… IAPT dataset’ (ibid., comment 8) and therefore does not even follow ‘NICE’s own procedural manual’ (ibid.). As Loewenthal puts it: ‘whilst [NICE] recognises many of the issues concerning its methodology, it ends up acting as if they don’t exist’ (Loewenthal, 2016, p.18). Loewenthal (2016) suggests that therapy’s historical and contemporary practices of supervision, writing and presenting papers provide a functional way of monitoring and evaluating practice which is superior to RCTs which he asserts are ‘against the very nature of what for many is the therapeutic enterprise’ (p. 14). He perceives the emphasis on RCTs, and similar forms of privileged quantitative research, shaping practice detrimentally, and mourns ‘[t]heoretical explorations’ not being seen as research at all. He cites the APA’s encouragement of a pluralistic approach to research methodologies to suggest a way forward for NICE and IAPT, whose over-adherence to a medicalised symptom-based model constructs versions of therapy, and ways of researching therapy, which can only be useful for therapists and clients if they are in agreement that the latter’s problems fit neatly into diagnostic labels. Real consequences of the monistic, quantitative and scientistic approach to approving therapies are that choices for NHS patients are, self-evidently, limited to the approaches that have been approved, and therapists, some with decades of clinical practice and experience, who have not trained in these approved practices, are perceived as having nothing to offer. This issue has been highlighted by research undertaken by the BACP (Perfect et al., 2016) in their document Choice of Therapies in IAPT: An overview of the availability and client profile of step 3 therapies. Barkham et al. (2017) also make the point that ‘improving patient treatment choice improves therapy outcomes’ (ibid., p. 264), so reducing choice is counter-productive. Additionally, despite the success of Counselling for Depression (CfD) in RCTs leading to it being nominated by NICE as an ‘evidence-based’ therapy, CfD practitioners only make up ‘6% of the high-intensity therapist workforce’ (Drewitt et al., 2018). In other words, even providing the required evidence does not seem to have made much impact in improving choice of different therapies for clients.
The biggest change affecting the provision of therapy in the UK was the formation of IAPT. This has been dated to 2003 when Lord Layard met Professor David M. Clark at a British Academy tea party (Evans, 2013). From a symbolic interactionist perspective it is notable that perhaps the most important development in the provision of therapy in the UK this century occurs in a microsocial context.
On one level, the introduction of IAPT, when it came, was a giant leap for the provision of therapy in Britain, as ‘[b]efore IAPT, the NHS spent just 3% of its mental health budget on talking therapy’ and ‘IAPT… tripled that budget’ (ibid.). However, with the publication of the NICE guidelines for depression in 2004, it was disappointing for therapy professionals that only two types of therapy were recommended – namely, CBT and a time-limited, structured therapy called interpersonal therapy (IPT). All other approaches were not recommended for depression because, according to NICE’s definition of evidence, all other approaches did not have enough to gain the status of ‘evidence-based’. Even accepting that therapeutic approaches should be seen as targeting specific disorders, and prove their effectiveness at targeting them, the guidelines were problematic, as the evidence was clearer for ‘severe’ as opposed to ‘mild’ or ‘moderate’ depression. Therefore a potential danger, recognised by medical professionals themselves, was that clinicians/patients might take on a more serious ‘depression’ diagnosis in order to obtain treatment that would not be available with a less serious or non-medicalised complaint. However, the evidence of what worked for mild or moderate depression was not as robust so, ultimately, there was not sufficient evidence that people with mild or moderate depression were actually getting evidence-based treatment (Middleton et al., 2005).
In January 2005, Layard and Clark presented their recommendations at 10 Downing Street, and proposals for IAPT went into the Labour Party’s manifesto for the 2005 general election (Evans, 2013; Cohen, 2008). One major reason that Layard and Clark were able to get the Labour government to commit to an IAPT programme was because ‘CBT had built up a big evidence base to show it worked’ (Evans, 2013, online; see also Research Excellence Framework, 2014) – although the superiority of CBT to counselling and other psychological therapies is easily disputed (e.g. Barkham et al., 2017). When what has come to be known as Layard’s ‘Depression Report’ came out in 2006, CBT was recommended as a therapeutic approach that would not just be effective, but also inexpensive and efficient (CEPMHP, 2006). In the report CBT was described as the ‘most developed of [the evidence-based psychological therapies]’ (p. 1). Of the 10,000 new therapists that they proposed should be trained in delivering CBT, they suggested that half of them should be ‘clinical psychologists’, and the other half trained from the existing workforce of ‘nurses, social workers, occupational therapists and counsellors’ (p. 7). It is interesting to note that counsellors are enumerated last in that list, and their expertise in delivering therapy only acknowledged as equivalent to the other professions that precede their mention. Psychotherapists receive no mention at all. This powerful document, whose effects are still reverberating around the provision of therapy in the NHS, effectively discounted the expertise of therapists (both psychotherapists and counsellors) already working in the NHS, and the models they had trained in, as insufficient for the task of ‘improving access’ to psychological therapies. Documents like this came to create a cultural ground in which CBT became privileged as the best therapeutic approach at the expense of others. Perhaps the only ‘winners’, in terms of increased employment opportunities and power, were psychologists associated with CBT: recent figures (IAPT’s own) state that 42 per cent of the IAPT workforce are CBT practitioners (Drewitt et al., 2018).
Therefore, in the sociohistorical developments of the therapy profession in the UK, a trajectory can be traced from competing interests within the profession itself, leading to an emphasis on research which then leads to an emphasis on the RCT. In response to the context of a developing audit culture and that culture’s need for evidence and efficiency, CBT, with its evidence base and perceived efficiency, then comes to dominate the provision of therapy, and other approaches lose their status and are marginalised, if not erased, from public providers. The private sector, EAPs, insurance companies and the third sector continued to provide employment opportunities for other approaches but, within the NHS, CBT, to a great extent, began to monopolise therapy provision.
The dominance of CBT and the marginalisation of other types of counselling and psychotherapy is one of the biggest, most frustrating problems facing current practitioners and of course, clients, who cannot access what these therapists provide even if they know it is what they want. You could say CBT has been the flavour of the past decade in the NHS and beyond. In terms of public relations it has made great achievements in influencing the media, usually uncritically, to accept it as the only evidence-based therapeutic approach for a wide array of ‘disorders’. Simultaneously it has come under attack from therapists who do not follow the approach, perhaps with some rationality, but also with emotional defensiveness (e.g. Leader, 2008). For therapists who do not follow the approach, and have belief in the efficacy of their own non-CBT approaches, it can seem like watching helplessly as one pupil gets all the prizes.
A common critique of CBT, articulated in different ways, is that it reflects a wider neoliberal agenda in which teaching ‘“technologies of the self” to the CBT patient echo Foucault’s notion of “disciplinary power”… where the state uses subtle power to mould its subjects into acquiescence’ (Watts, 2016, p. 89). Unsurprisingly, CBT practitioners and their proponents rebuff these kinds of criticisms as a caricature (e.g. Veale, in Samuels & Veale, 2009).
In 2008, adding to the plurality of psychological practitioners, the DH produced an implementation plan for the training of ‘low-intensity therapies workers’ who would facilitate the use of CBT via ‘guided self-help and computerised CBT’ (Department of Health, 2008, p. 3). These workers would come to be known as ‘Psychological Wellbeing Practitioners’ (PWPs) who would be perceived as fit to practise after 45 days training (ibid.). One advantage, in terms of cost, is that these practitioners could expect a maximum pay rate less than even a trainee psychotherapist. Therefore therapists in the NHS were not only coming under pressure in terms of their approaches being devalued, but also in terms of their professional opportunities being ‘undercut’ by the creation of jobs/titles purportedly needing less expertise and a ‘proletarianisation’ of therapeutic practice.
It is against this background of an audit culture which based its decisions about therapy provision on narrow definitions of evidence that led to the monistic hegemony of CBT in the NHS and the pushing away of counsellors and psychotherapists into other sectors.
References
BACP (2017a). BACP response to NICE: Depression in Adults: Recognition and Management consultation on draft guideline. Accessed at https://www.bacp.co.uk/media/2275/bacp-response-nice-guidance-depression-in-adults.pdf on 6 March 2018.
Barkham, M., Moller, N.P. & Pybis, J. (2017). How should we evaluate research on counselling and the treatment of depression? A case study on how the National Institute for Health and Care Excellence’s draft 2018 guideline for depression considered what counts as best evidence. Counselling & Psychotherapy Research, 17(4). 253–268.
CEPMHP (The Centre for Economic Performance’s Mental Health Policy Group). (2006). The Depression Report: A New Deal for Depression and Anxiety Disorders. Centre for Economic Performance, London School of Economics. Accessed at eprints.lse.ac.uk/818 on 15 November 2017.
Cohen, A. (2008). IAPT: A brief history. Healthcare Counselling & Psychotherapy Journal, April. 8–11.
Department of Health. (2008). Improving Access to Psychological Therapies: Implementation Plan: Curriculum of Low-Intensity Therapies Workers. London: Department of Health.
Drewitt, L., Pybis, J., Murphy, D. & Barkham, M. (2018). Practitioners’ experiences of learning and implementing Counselling for Depression (CfD) in routine practice settings. Counselling & Psychotherapy Research, 18(1). 3–13.
Evans, J. (2013). A brief history of IAPT: The mass provision of CBT in the NHS. Accessed at https://emotionsblog.history.qmul.ac.uk/2013/05/a-brief-history-of-iapt-the-mass-provision-of-cbt-in-the-nhs/on 11 November 2016 (originally posted 30 May 2013).
Leader, D. (2008). A quick fix for the soul? Guardian, 9 September. Accessed at https://www.theguardian.com/science/2008/sep/09/psychology.humanbehaviour
Loewenthal, D. (2016). Therapy as cultural, politically influenced practice. In J. Lees (Ed.), The Future of Psychological Therapy: From Managed Care to Transformational Practice. Abingdon: Routledge.
Middleton, H., Shaw, I., Hull, S. & Feder, G. (2005). NICE guidelines for the management of depression: Are clear for severe depression, but uncertain for mild or moderate depression. British Medical Journal, 350. 267.
NICE. (2016). History of NICE. Accessed at https://www.nice.org.uk/about /who-we-are/history-of-nice on 11 November 2016.
NICE. (2014 / updated 2017). Developing NICE guidelines: the manual: process and methods. Accessed athttps://www.nice.org.uk/process/pmg20/chapter/introduction-and-overview on 4 July 2018.
Perfect, D., Jackson, C., Pybis, J. & Hill, A. (2016). Choice of therapies in IAPT: An overview of the availability and client profile of step 3 Therapies. Lutterworth: British Association for Counselling & Psychotherapy.
Research Excellence Framework. (2014). Improving policy and practice to promote better mental health. Accessed at http://impact.ref.ac.uk/CaseStudies/CaseStudy.aspx?Id=40639# 6 September 2017.
Sackett, D.L., Rosenberg, W.M., Gray, J.A.M., Haynes, R.B. & Richardson, W.S. (1996). Evidence based medicine: what it is and what it isn’t. British Medical Journal, 312. 71–72.
Samuels, A. & Veale, D. (2009). Improving access to psychological therapies: For and against.Psychodynamic Practice, 15(1). 7–24.
Wampold, B.E. & Imel, Z.E. (2015). The Great Psychotherapy Debate: The Evidence for What Makes Therapy Work, 2nd Edn. Hove: Routledge.
Watts, J. (2016). IAPT and the ideal image. In J. Lees (Ed.), The Future of Psychological Therapy: From Managed Care to Transformational Practice. Abingdon: Routledge.
Jay Beichman is a member of the uACT organising group.

{kind=link}